Skyra 3 tesla magnetom running in the neurosuite since
28-November-2013
CEREBELLOPONTINE ANGLE MENINGIOMAS
Management
These meningiomas may arise from any area of the dura on the posterior
surface of the petrous bone. At operation four general categories of tumor
are found, depending on where they arise and their relationship to the
seventh and eighth nerve complex:
1. Anterior to the internal auditory meatus, displacing the seventh and
eighth nerves posteriorly and inferiorly (as the case 1 demonstrated below).
2. Between the internal auditory meatus and the jugular foramen, displacing
the seventh and eighth nerves superiorly.
3. Superior to the internal auditory meatus, displacing the seventh and
eighth nerves anteriorly in the large tumors.
4. Surrounding the internal auditory meatus, with the seventh and eighth
nerves engulfed in the tumor. MRI of Meningioma
FIG.1. Cerebellopontine angle meningioma. This 47-year-old woman had
progressively decreased hearing in her left ear and discomfort around her
ear and the side of her head. Total removal of the tumor was done using a
subtentorial supracerebellar approach. There was normal recovery. MRI axial
TI images after gadolinium show a large meningioma arising posterior to the
left internal auditory meatus.
The MRI scan usually defines those tumors that arise posterior to the
internal auditory meatus but will not distinguish the first three
categories. The diagnosis of meningioma is indicated by the flat surface of
the tumor against the petrous bone and the dural "tail" extending from the
tumor.
MRI usually gives all the information needed and in most patients. The blood
supply comes primarily through the dural attachment. Embolization has not
been a consideration.
In patients with mild or minimal symptoms, an initial period of clinical
evaluation and repeat scans may be indicated to determine whether there are
progressive symptoms and an enlarging tumor. This is especially true in the
elderly.
The indications for operation are a worsening neurological deficit due to
brainstem compression or cranial nerve compression. In a few patients
headache or the continued presence of a stable deficit such as diplopia or
hearing loss may be the indication.
The key considerations in the operation include:
Exposure of the tumor. Interruption of the blood supply along the dural
attachments. Internal decompression combined with careful dissection of the
tumor capsule from the brainstem and cranial nerves.
Postoperative complications included permanent increased ataxia, due to a
cerebellar infarction or wound infection and meningitis and cerebrospinal
fluid leak requiring repair. Several patients had temporary increases in
ataxia, incoordination, or swallowing problems which improved. Around 10%
patients had a shunt for hydrocephalus at some time in their course.
Yasargil et al. reported that 27 of 30 patients had a good result and in 27
the tumor was "radically excised." Sekhar and Jannetta reported total
removal in 14 of 22 patients, with no operative mortality and a good outcome
in 16. Samii and Ammirati reported total removal of all 24 tumors
located posterior to the internal auditory meatus, with a good outcome for
22 patients. Of 32 patients with tumors anterior to the internal auditory
meatus, 29 had the tumors totally removed and 28 had a good outcome.
After careful positioning, the patient's head is held with the three-point skeletal fixation headrest. Care is taken to keep the head above the heart level and to avoid compression of the jugular veins in the neck. The position must take into account the effects of gravity, the need to minimize brain retraction, and the avoidance of compression of the brain against the edge of the dura. If the head is to be well elevated or a semisitting position is used, a central venous pressure line is placed in the right atrium, using x-ray guidance. Some type of magnification (either loupes or the operating microscope) is used for the entire operation. The skin incision must allow for full exposure of the tumor. Blood supply to the scalp flap must be adequate. and a wide enough base must be left to provide good vascularization. The cosmetic result of the scar and bone flap should be considered. The pericranial tissue is left attached to the back of the scalp flap so it can be taken at the end of the operation to repair any dural defects. A free bone flap will allow wide. expeditious exposure of tumor and can be easily enlarged if necessary. Blood supply coming through the bone is occluded. At the end of the operation the bone flap is wired solidly in place. If burr holes or bone removal due to tumor will leave a cosmetic deformity or a large bone defect. a cranioplasty is done. For a burr hole or small bone defect, the area is filled with acrylic or bone dust harvested during burr hole production.
Bleeding from the dura is controlled with bipolar coagulation. Surgicel or Gelfoam. The dura is held to the inner table of bone along the craniotomy opening with sutures placed from dura to pericranial tissue or into holes drilled in the bone.
For superficial meningiomas the dura is opened at the margin between brain and tumor. One should always try to expose as little normal brain as possible. especially when the brain is still full because of the presence of a large tumor mass. All dura attached to the tumor is eventually removed. but in convexity and parasagittal meningiomas it is usually wise to leave it attached to help in retraction. At the end of the operation the convexity dura is replaced with a graft of pericranial tissue which is taken from the back of the scalp nap.
Everything is done to avoid retraction or removal of adjacent brain tissue. In many patients it is best to carry out an extensive internal decompression of the tumor prior to trying to dissect the capsule. The decompression is facilitated by use of the ultrasonic aspirator or cautery loops. Bleeding from within the tumor will often cease spontaneously. but in some cases bipolar coagulation or Surgicel may be needed. Gentle pressure is placed against the capsule of the tumor or on the dural attachment to help define the plane with adjacent brain tissue. Brain tissue is gently separated from the capsule of the tumor using fine dissectors. As blood vessels between capsule and brain tissue are encountered. they are coagulated with bipolar coagulation and cut with microscissors.
The overall operative mortality in supratentorial meningiomas is less than 1 percent. Malignant meningiomas are considered separately.
Case 1.
09-FEBRUARY-2014 SAMIRA FAZEH ABU-DARWEESH 49 YEARS LEFT CPA GIANT
MENINGIOMA.
Anamnesis
The patient came to the clinic 03-February-2014 complaining of left sided
headache for 28 years and considered as having migraine with exacerbation
the last month. MRI of the brain of bad quality done at Al-Bashir hospital
12-October-2011 reported to be normal, but there was a lesion in the left
CPA. The last month has ataxic gait. Numbness of the left side of the face
and the the tongue. The patient is left handed. Sialorrhea from the left
side.
On examination; the patient is alert is responding to all verbal responses.
She has hypalgesia of the left side of the face. Romberg stable. The hearing
decreased in the left side with tinnitus left ear for 4-5 months. There is
weak right upper and lower limbs right side 4/5. Hoffmann was positive in
the right. Babinski and clonus of the right foot ?.
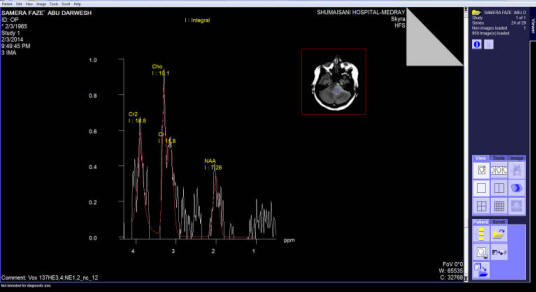
The patient sent for new MRI of the brain with contrast and spectroscopy.
All data were in favor of huge left CPA meningioma 33x32x30 mm dimension.
MRA showed compression of the basilar artery with the corresponding PICA by
the tumor mass. Spectroscopy was typical of meningioma.
Setting position. Craniotomy done to expose the left cerebellar hemisphere
and the left transverse sinus and abutting the left sigmoid sinus. The dura
was opened to reach the subtentorial area. The meningioma was seen at the
most anterior parts. The tentorium was not involved by the matrix of the
tumor, nor the superior petrosal sinus. The tumor was rubbery in consistency
with good cleavage. Piece meal resection was started and the tumor was
dissected off the brain stem, cerebellar hemisphere. After total resection
of the tumor, the trigeminal nerve was pushed upward flattened and stuck
with the brainstem. The facial and vestibulo-cochlear nerves were pushed
down and posterior. The left AICA and its branches were preserved. The tumor
matrix was superior to the meatus acousticus internus. Some feeders were
coagulated to achieve Hemostasis. Further hemostasis was achieved by
applying surgicele. The patient was sent to MRI to confirm the total
resection of the tumor. There is no any residual mass, except the surgicele.
The patient now in supine position and routine closure of the wound.
Smooth postoperative recovery. The facial and all the nerves of the area are
functioning properly. Sent to the ICU.
Postoperative course:
The patient complained of double vision when looking to the left. It could
be explained by the reaction of the quadrigeminal structures after tumor
removal.
The final histologic result was fibroblastic meningioma.
Comments
The patient underwent intraoperative MRI to confirm the radical resection of
the tumor. The good shape of the brainstem, gave the decision, that the
patient can be extubated immediately after surgery and this was achieved.
The essential purpose of intraoperative MRI control is to catch any
complication during surgery and to know exactly what happened and to respond
accordingly.
The patient was operated in setting position during tumor removal, but the
surgery was continued after MRI control in supine position. A massive
bleeding took place from the intraoseous veins from the bone defect. The
conclusion is that it is mandatory to wax all the bone edges for 2 reasons.
First the prevent the progression of air embolism, second: to prevent
postoperative extradural bleeding.
Spectroscopy of the meningioma, which proved to be fibroblastic meningioma.