Skyra 3 tesla magnetom running in the neurosuite since
28-November-2013
Extracranial meningiomas of the head and neck region are rare neoplasms, the
majority being a secondary location of a primary intracranial tumour.
Prognosis of this tumour is generally excellent.
Surgical excision is the treatment of choice, with no need for further
treatment; nevertheless, differential diagnosis must consider other more
common tumours of the head and neck and be based on histopathologic
examination and relative techniques, including examination of frozen
sections. This procedure is particularly useful assessing surgical treatment
and should be performed whenever possible to exclude the malignant nature of
the lesion and avoid over-treatment.
Introduction
According to the World Health Organization, meningioma is a tumour arising
from arachnoidal cells and, in the majority of cases, its behaviour is
benign. It accounts for 24-30% of all intracranial tumours and has an
incidence of 13/100,000 per year.
Extracranial meningiomas are rare; the majority have a secondary location of
a primary intracranial tumour. Therefore, once the diagnosis of meningioma
is established, the presence of a meningioma of the neuraxis or extension of
a primary central meningioma must be excluded.
Case demonstration:
The patient came to the clinic 29-April-2014 complaining of difficult
breathing fro the right nostril with progressive exophthalmus right eye for
one year. He was operated for septal deviation elsewhere without benefit.
CT-scan done 29-April-2014 showing a huge mass in the right maxillo-
sphenoidal area, pushing the septum to the left and elevating the medial
wall of the right orbit up and lateral.
On examination; the patient has no visual problems except the right
exophthalmus. The lacrimal duct is closed and the tears are running outside
the canal. It was possible to see the tumor through the right nostril. It
was totally obstructing the passage.
The patient was sent for MRI investigations with contrast with MRA of the
brain and carotid systems. There was no arterial involvement and the mass
was totally extracranial, but reaching and abutting the pituitary floor and
shifting the right optic nerve medially.
Through the right nostril, the tumor was attacked and piece-meal resection
was performed. Fresh frozen biopsy telling that it is either meningioma or
fibrous dysplasia. Inspection of the tumor bed cavity was negative.
Intraoperative MRI done showing huge remnant of the tumor, which was
followed and resected. Hemostasis. 2 nasal tubes were inserted.
Smooth postoperative recovery.
The patient is not characteristic for either meningioma, nor for fibrous
dysplasia. It is benign and grossly looking as chordoma.
Intraoperative MRI is superior to the usual inspection, as in this case.
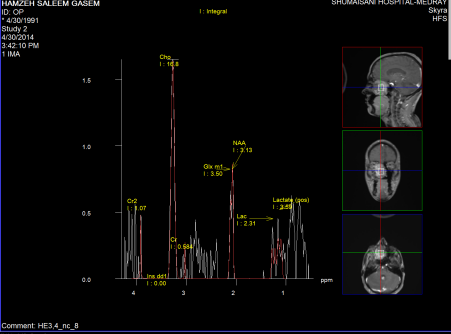
Figure-1
Figure-2
In retrospective analysis of the MR Spectroscopy done before surgery, it was
similar to pattern seen intracranially as seen in Figure 1 and 2.
Discussion
Primary extracranial meningiomas of head and neck region are rare tumours,
the majority being a secondary location of a primary intracranial tumour,
accounting for 1-2% of all meningiomas and with a generally favorable
prognosis.
Therefore, once the
diagnosis of meningioma is established, the presence of a meningioma of the
neuraxis or extension of a primary central meningioma should be excluded.
The most frequent extracranial sites reported are the nasal cavity and
paranasal sinuses, cranial bones, middle ear, scalp and soft tissues of the
face and neck and parotid gland. The largest series of extracranial head and
neck meningiomas encompass 146 cases, among which the majority was of the
skin and scalp (n = 59), middle ear (n = 26), nasal cavity (n = 17),
temporal bone (n = 2) and parotid gland (n = 1). Other large series consider
the sinonasal tract (n = 30) 6, ear and temporal bone meningiomas.
The etiology of extracranial meningiomas resides in the migration of
arachnoid cells deriving from the neural crest, but different mechanisms
have been proposed such as originating from arachnoid cells of nerve sheaths
emerging from skull foramina, from Pacchionian bodies possibly displaced or
entrapped in an extracranial location during embryologic development, by
trauma or cerebral hypertension displacing arachnoid islets or deriving from
undifferentiated mesenchymal cells.
Extracranial meningiomas exhibit various different histologic patterns just
as their intracranial counterparts.
By cytology, meningotheliomatous cells show bland nuclei with delicate
chromatin and intranuclear pseudoinclusions. The immunohistochemical profile
of extracranial meningiomas is indistinguishable from intracranial lesions.
All tumours expressed epithelial membrane antigen and vimentin, variable
expression of protein S-100 and are negative for acidic gliofibrillary
protein.
Although the lesions has a radiographic and histological growth pattern that
is aggressive, none were diagnosed as a malignant meningioma. Their indolent
clinical behaviour was further suggested by cellular immunoreactivity for
Ki-67, which was less than 5%. Differential diagnosis includes different
benign and malignant tumours, such as epithelial neoplasms (carcinoma),
tumours originating from the neural crest (melanoma, olfactory neuroblastoma)
and vascular and mesenchymal tumours (angiofibroma, paraganglioma, ossifying
fibroma).
Histologic features and immunohistochemical findings can easily separate
these entities, especially in the differential diagnosis between carcinoma
and melanoma; in more intriguing cases immunohistochemistry for cytokeratins,
S-100 protein and HM B-45 allows distinction from meningiomas.
Prognosis of primary meningioma is generally excellent, thus supporting the
indolent growth of meningiomas, except for rare malignant forms; surgical
excision is the treatment of choice, with no need for further treatment.
Recurrences usually develop in the same site as the primary lesion and
probably represent residual disease rather than recurrent tumour.
Clinical and radiographic features of these tumours cannot predict the
nature of these lesions. Therefore, histopathologic examination is necessary
as it can distinguish these
neoplasms from other head and neck tumours. In particular, frozen sections
are particularly useful in assessing the surgical procedure and should be
performed whenever possible to exclude the malignant nature of the lesion
and avoid overtreatment.